Most people have never heard of the pterygoid process — and that is completely understandable. It is a small bony projection tucked deep inside the base of the skull, invisible to the naked eye and unknown to anyone outside clinical anatomy. Yet despite its modest size, it plays a significant role in how you chew food, speak clearly, and swallow without a second thought.
Every time you bite into something, a complex chain of muscular and skeletal events fires off in milliseconds. The jaw opens, the muscles contract, the teeth come together — and at the very center of all that mechanical coordination sits a region of the skull that surgeons, dentists, and anatomists have studied for centuries.
Understanding its anatomy is not purely academic. Dentists rely on it when planning complex implant procedures. Surgeons reference it during skull-base operations. Radiologists trace it on CT scans to diagnose trauma. ENT specialists navigate around it during endoscopic procedures. In short, this bony structure shows up constantly in clinical medicine — and this article will walk you through exactly why.
What Is the Pterygoid Process and Where Does It Sit?
The pterygoid process is a paired bony projection that extends downward from the junction of the body and greater wing of the sphenoid bone. There is one on each side of the skull — left and right — positioned symmetrically at the base of the cranium.
The sphenoid bone sits at the very center of the skull base, wedged between the frontal, parietal, temporal, and occipital bones. It is often called the “keystone” of the cranial floor because it articulates with so many neighboring bones. Its lower surface features two bony projections hanging downward like inverted wings, pointing toward the roof of the mouth.
Each process is made up of two vertical plates of bone — the medial plate and the lateral plate — separated by a depression called the pterygoid fossa. These two plates are not identical. They differ in shape, size, and the structures they anchor. Together, they create a bony framework that supports the muscles responsible for chewing, soft-palate movement, and jaw stability.
The Pterygoid Canal — A Hidden Passageway
Running through the root of each process is a narrow bony tunnel called the pterygoid canal, also known as the Vidian canal. This canal carries the Vidian nerve — a combined nerve that brings together sympathetic fibers from the deep petrosal nerve and parasympathetic fibers from the greater petrosal nerve. These fibers travel forward to the pterygopalatine ganglion, which sits just ahead of the process in the pterygopalatine fossa. This ganglion controls glandular secretion in the nasal cavity, palate, and lacrimal gland, making the pterygoid canal far more important than its small size suggests.
Breaking Down the Structure of the Pterygoid Process
The internal architecture of this sphenoid bone projection is worth studying carefully. Each half consists of two plates, a fossa, and several smaller but clinically important features. Here is a detailed look at each component.
The Lateral Plate of the Pterygoid Process
The lateral plate of the pterygoid process is broader and shorter compared to the medial plate. Its outer surface faces the infratemporal fossa — the space below the temporal fossa and behind the maxilla. Its inner surface faces the pterygoid fossa.
This plate serves as a direct attachment site for two powerful chewing muscles. The lower head of the lateral pterygoid muscle originates from its outer surface. The deep head of the medial pterygoid muscle originates from the inner surface — specifically from the pterygoid fossa between the two plates. This dual muscular attachment makes the lateral plate a true mechanical anchor for jaw function.
When this plate is fractured — as can happen in high-energy facial trauma — both muscles lose their bony anchorage. The result is predictable: restricted jaw movement, malocclusion, and significant pain.
The Medial Plate and the Pterygoid Hamulus
The medial plate is longer and narrower than the lateral one. Its lower end curves into a hook-like bony projection called the pterygoid hamulus — one of the more distinctive structures in skull anatomy. The tendon of the tensor veli palatini muscle wraps around this hamulus like a pulley before fanning out into the soft palate.
This mechanical arrangement allows the muscle to apply tension evenly across the palate, which is essential for functions like swallowing and equalizing ear pressure when you yawn. When the hamulus is disrupted — whether through fracture, surgical damage, or abnormal bone growth — patients often report difficulty swallowing, a sensation of something catching in the throat, or persistent ear pressure that does not resolve.
The Pterygoid Fossa and the Scaphoid Fossa
Between the medial and lateral plates lies the pterygoid fossa. This concave space provides a surface for the origin of the medial pterygoid muscle — specifically its deep head. Just above this fossa, at the superior border of the posterior edge of the medial plate, lies a small depression called the scaphoid fossa. This is where the tensor veli palatini muscle begins before its tendon descends to wrap around the hamulus. It is a subtle anatomical detail, but surgeons operating in this region must be familiar with it.
Muscles That Originate From the Pterygoid Process
Two of the four muscles of mastication attach directly to this region. Their function, position, and clinical relevance make them among the most discussed muscles in dental and maxillofacial medicine.
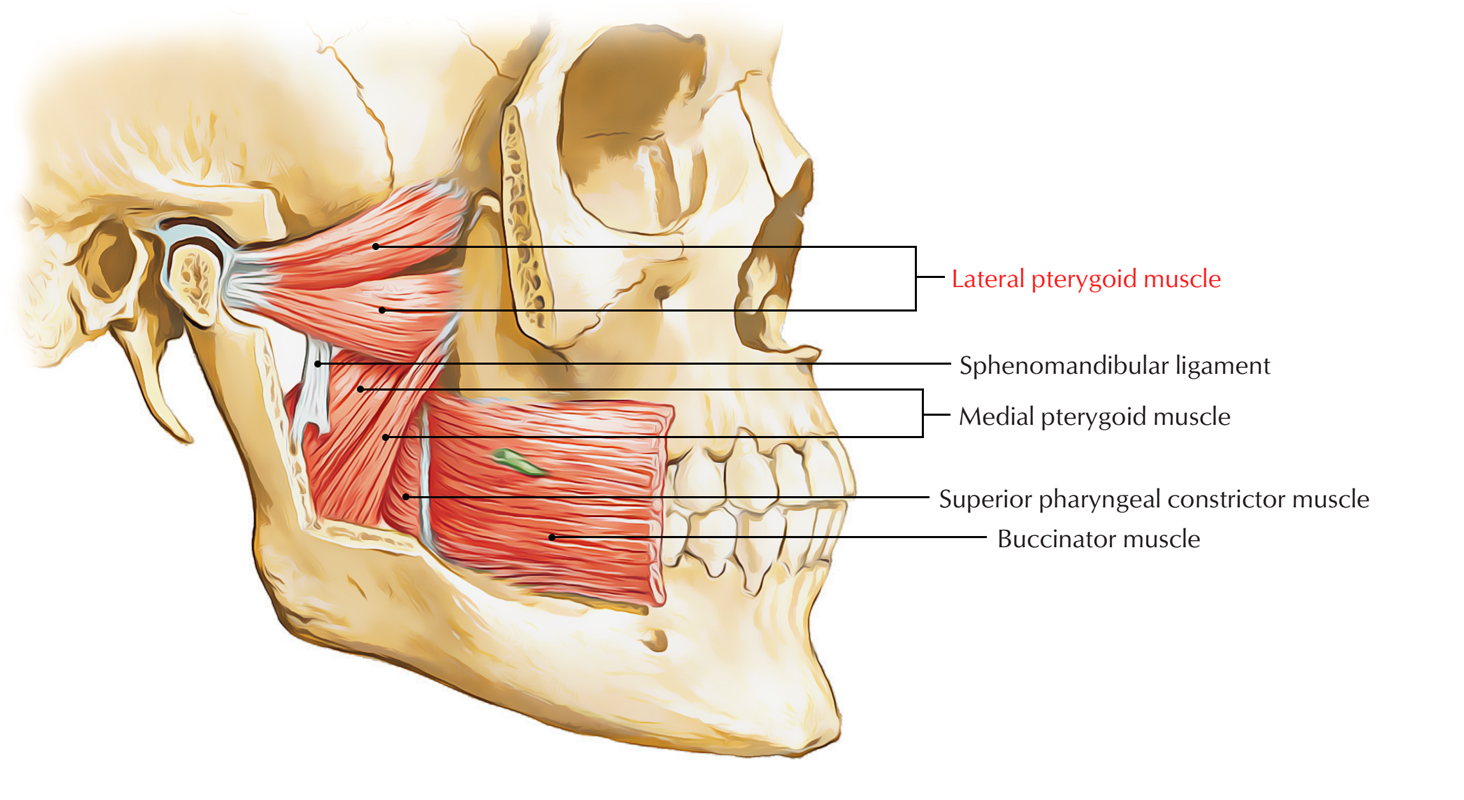
The Lateral Pterygoid Muscle
The lateral pterygoid is a short, thick, two-headed muscle that runs nearly horizontally. Its upper head originates from the infratemporal surface of the greater wing of the sphenoid, while its lower head originates from the lateral plate described above. Both heads insert into the neck of the mandibular condyle and the articular disc of the temporomandibular joint (TMJ).
This muscle is primarily responsible for opening the mouth. When both sides contract simultaneously, they pull the condyles forward, protracting the mandible. When one side contracts alone, the jaw shifts laterally — essential for the grinding motion involved in chewing. Because of its direct insertion into the TMJ disc, the lateral pterygoid is heavily implicated in TMJ disorders, disc displacement, and jaw clicking.
The Medial Pterygoid Muscle
The medial pterygoid runs obliquely downward and backward from the pterygoid fossa. It inserts into the medial surface of the mandibular ramus and angle. Its function is essentially the opposite of the lateral pterygoid — it closes the jaw by elevating the mandible.
Together with the masseter muscle, it forms a muscular sling around the angle of the mandible. This sling generates impressive force relative to its size. Dysfunction here — from trauma, abscess, or surgery — causes trismus, a painful and often alarming inability to open the mouth fully.
Nerves Passing Through and Around the Pterygoid Region
Several important nerve branches travel through and around this area, making anatomical knowledge here critical for anyone performing injections, surgery, or interpreting facial pain patterns.
The Vidian nerve travels through the pterygoid canal at the base of the process, carrying secretomotor fibers to the nasal mucosa, palate, and lacrimal gland. In cases of intractable allergic rhinitis, surgeons sometimes cut this nerve — a procedure called a Vidian neurectomy — by approaching through the nose endoscopically.
The mandibular nerve (V3), the third division of the trigeminal nerve, exits the skull through the foramen ovale and descends into the infratemporal fossa directly adjacent to the lateral plate. Its branches — including the inferior alveolar nerve, lingual nerve, and buccal nerve — course through spaces bounded in part by the pterygoid structures. This is precisely why a pterygomandibular nerve block, commonly used in dentistry to numb the lower jaw, is performed using the medial plate as a tactile landmark.
The pterygopalatine ganglion hangs from the maxillary nerve in the pterygopalatine fossa, just medial and anterior to the bony process. It receives its parasympathetic input through the Vidian nerve and distributes fibers to the nasal cavity, sinuses, palate, and orbit. Pain specialists sometimes target this ganglion for nerve blocks to manage severe facial pain conditions.
Why the Pterygoid Process Matters in Dentistry and Oral Surgery
Few regions of skull anatomy have seen as much growth in clinical relevance over the past two decades. The pterygoid process of sphenoid bone has become a key target in implant dentistry — particularly for patients who have lost significant bone in the back of the upper jaw.
Pterygoid Implants in Full-Arch Rehabilitation
When the posterior maxilla has resorbed severely, placing standard dental implants there becomes nearly impossible without extensive bone grafting. Pterygoid implants — also called tuberopterygoid or pterygomaxillary implants — offer a solution. These are long, angled implants that engage the pterygoid plates and the pyramidal process of the palatine bone, bypassing compromised maxillary bone entirely.
Studies have reported high survival rates for pterygoid implants, often exceeding 90% at five-year follow-up. They allow full-arch prosthetic rehabilitation without bone grafts, reducing surgical time, cost, and recovery. But they require precise 3D planning and a thorough grasp of regional anatomy — especially the angulation and density of the lateral plate.
Pterygomandibular Space and Third Molar Surgery
The pterygomandibular space — bounded medially by the medial pterygoid muscle and laterally by the mandibular ramus — is an area dentists navigate every time they perform lower wisdom tooth extractions or inferior alveolar nerve blocks. Swelling or infection in this space can spread rapidly to adjacent fascial spaces, making it a clinically dangerous region when complications arise.
Fractures and Pathologies of the Pterygoid Region
Trauma is one of the most common reasons this bony area becomes a focus of clinical attention. Fractures here tend to occur in the context of broader craniofacial injuries.
Fractures in Le Fort Injuries
The classic Le Fort classification of midface fractures includes these bony structures as a defining anatomical feature. In Le Fort II and Le Fort III fractures — which involve progressively higher levels of midface separation — both are fractured as part of the injury pattern. A floating midface without this involvement simply cannot occur by definition.
Patients with these injuries present with facial swelling, mobility of the midface, malocclusion, and sometimes severe nosebleeds. CT scanning with fine cuts through the skull base is the standard diagnostic tool. Treatment involves surgical reduction and internal fixation, typically using titanium plates and screws.
Nasopharyngeal Carcinoma and Skull-Base Invasion
Nasopharyngeal carcinoma frequently spreads laterally toward the pterygoid region. When the tumor invades the pterygoid musculature or erodes into the bony plates, it causes deeply painful and persistent trismus. This symptom — jaw stiffness and restricted opening — is sometimes the first clinical sign that prompts further investigation. MRI is the preferred imaging modality for soft-tissue involvement in this area.
Juvenile Nasopharyngeal Angiofibroma
This highly vascular, benign tumor typically affects adolescent males. It commonly extends into the pterygopalatine fossa and can erode into this bony root as it expands. Surgical resection requires meticulous preoperative planning due to the risk of severe bleeding, and embolization of feeding vessels is typically performed beforehand.
Fibrous Dysplasia
Fibrous dysplasia is a benign bone condition in which normal marrow is replaced by fibrous tissue. When it involves the sphenoid, it can expand into the pterygoid region, distorting the plates and potentially compressing neural structures passing through the Vidian canal.
Identifying This Structure on CT and MRI Scans
Radiologists and surgeons who work in the skull base develop fluency with the imaging appearance of this region early in their training. On axial CT slices, the two plates are easily identifiable at the level of the inferior sphenoid. The lateral plate appears as a broader bony shelf, while the medial plate is thinner and hooks medially at its inferior end — forming the hamulus.
On coronal cuts, the pterygoid fossa between the two plates appears as a V-shaped notch open inferiorly. The pterygoid canal is best visualized on axial cuts just above the level of the plates, running anteroposteriorly through the base of each bony process.
MRI adds soft-tissue context that CT cannot. The pterygoid muscles, the contents of the pterygopalatine fossa, and the Vidian nerve can all be visualized with appropriate sequences. For evaluating tumor extension or perineural spread, MRI with contrast is indispensable.
The Pterygoid Process Across Species — What Evolution Tells Us
In non-mammalian vertebrates such as reptiles, the pterygoid bone is a large, independent bone of the palate — not fused to the sphenoid. It forms a significant part of the roof of the mouth and often bears teeth in many species. Over the course of mammalian evolution, this separate bone became incorporated into the sphenoid complex, giving rise to the paired bony projections we see in modern human anatomy.
This evolutionary fusion explains why the region is so structurally and functionally complex. Herbivorous mammals with high masticatory demands — like horses and cattle — have particularly pronounced bony projections in this area to accommodate their powerful jaw-closing musculature. The human version is comparatively modest, but the structural logic is the same.
Surgical Procedures Involving the Pterygoid Region
This anatomical area is implicated in several well-established surgical approaches used in maxillofacial and skull-base surgery.
Le Fort I Osteotomy: This procedure, used to surgically reposition the upper jaw, involves cutting through the pterygomaxillary junction — the contact point between the maxilla and the pterygoid plates. A curved osteotome is used to disjoin the two structures, freeing the maxillary segment for repositioning. Incomplete separation here is one of the more common technical challenges in this surgery.
Vidian Neurectomy: Performed endoscopically through the nose, this procedure involves locating and cutting the Vidian nerve inside the pterygoid canal. It is used for patients with severe, treatment-resistant rhinitis. Precise anatomical knowledge of the pterygoid process of sphenoid is essential for surgeons performing this safely.
Infratemporal Fossa Approaches: For skull-base tumors extending into the infratemporal fossa, surgeons use lateral approaches that require controlled removal or displacement of the pterygoid plates to gain access to deeper structures.
Pterygomandibular Nerve Block: In everyday dental practice, the medial plate acts as a tactile guide. The needle is walked along the medial aspect of the mandibular ramus, just past the pterygomandibular raphe — a fibrous band anchored to the pterygoid hamulus — before depositing local anesthetic near the inferior alveolar nerve.
Final Thoughts on the Pterygoid Process
It is easy to overlook this structure — buried deep in the skull, rarely causing symptoms on its own, and absent from most casual conversations about anatomy. But once you understand how much depends on it, that oversight becomes hard to maintain.
Every chewing motion depends on muscles anchored to its plates. Every swallow involves a tendon wrapped around its hamulus. Every dental nerve block uses it as a physical guide. Every midface fracture involves it by definition. Every posterior maxillary implant may rely on it for long-term stability. The pterygoid process of sphenoid is not a footnote in skull anatomy — it is a central figure. For anyone working in dentistry, oral surgery, ENT, neurosurgery, or clinical anatomy, time spent understanding this structure is time very well invested.
FAQ 1: What is the pterygoid process? The pterygoid process is a paired bony projection that descends from the junction of the body and greater wing of the sphenoid bone at the base of the skull. Each process consists of a medial pterygoid plate and a lateral pterygoid plate, which serve as the origins of the medial and lateral pterygoid muscles. Wikipedia It is a key anatomical landmark in dental, surgical, and radiological practice.
FAQ 2: Where exactly is the pterygoid process located? Behind the third molar tooth lie two pterygoid processes, which extend downward from where the sphenoid bone’s body meets its greater wing. iMaios They sit on the undersurface of the cranial base, pointing downward toward the roof of the mouth — one on each side of the skull.
FAQ 3: What are the two plates of the pterygoid process? Each process has a medial and a lateral pterygoid plate that join towards the front but split apart at the back, forming a V-shaped space known as the pterygoid fossa. iMaios The medial plate is narrower and longer, while the lateral plate is broader and shorter, and each serves different muscular and functional roles.
FAQ 4: What is the pterygoid hamulus and what does it do? The medial pterygoid plate is narrower and longer than the lateral pterygoid plate, and it curves lateralward at its lower extremity into a hook-like process called the pterygoid hamulus, around which the tendon of the tensor veli palatini glides. Wikipedia This pulley-like arrangement enables the muscle to tension the soft palate for swallowing and ear pressure equalization.
FAQ 5: What muscles originate from the pterygoid process? The larger deep head of the medial pterygoid muscle originates from the medial surface of the lateral plate of the pterygoid process and the pyramidal process of the palatine bone. Kenhub The lower head of the lateral pterygoid muscle also originates from the lateral surface of the lateral plate, making this bony structure the shared anchor for two of the four muscles of mastication.
FAQ 6: What is the function of the lateral pterygoid muscle that attaches to this process? The lateral pterygoid muscle is active during mastication and mandibular movements — including protrusion (forward movement of the mandible), abduction (depression of the mandible), and mediotrusion (mandibular condyle movement towards the midline). NCBI It is the only muscle of mastication with horizontally arranged fibers, making it uniquely suited to opening and laterally shifting the jaw.
FAQ 7: What nerve passes through the pterygoid canal at the root of the pterygoid process? The Vidian nerve — formally the nerve of the pterygoid canal — passes through a bony tunnel at the base of the pterygoid process. The pterygopalatine fossa (PPF) communicates posteroinferiorly with the foramen lacerum through the pterygoid canal ScienceDirect, carrying both parasympathetic and sympathetic fibers to the pterygopalatine ganglion, which then controls nasal, palatine, and lacrimal gland secretion.
FAQ 8: Is the pterygoid process the same as the pterygoid bone? No — they are related but anatomically distinct. The anatomical term pterygoid process is derived from Greek and means “like a wing.” In many mammals it remains as a separate bone called the pterygoid bone. ScienceDirect In humans, this bone fused into the sphenoid during evolution, and what remains is the pterygoid process — no longer a separate bone, but a projection of the sphenoid.
FAQ 9: Can the pterygoid process fracture on its own without a Le Fort fracture? Yes, though it is rare. Approximately one-third of pterygoid plate fractures are unrelated to Le Fort fractures but are present alone or associated with other facial skeleton fractures. Digital Diagnostics Isolated fractures can occur from falls, direct blows, or even penetrating injuries and require CT imaging to diagnose accurately.
FAQ 10: How are pterygoid process fractures classified? Pterygoid process fractures are classified as: class I (vertical — simple separation between medial and lateral plates); or class II (transverse — with three subcategories according to the location of the fracture line relative to the pterygoid fossa and the sphenoid sinus floor). PubMed This classification guides surgeons in selecting the appropriate treatment approach.
FAQ 11: Are pterygoid process fractures always surgically treated? Not always. Le Fort fractures must be surgically treated with fixation of unstable fracture segments to re-establish bone form and function, and the pterygoid process must be surgically stabilized; however, surgical treatment is unnecessary in isolated pterygoid plate fractures. Digital Diagnostics Isolated cases are usually managed conservatively with pain control and monitoring.
FAQ 12: Can a lateral pterygoid plate fracture indicate a hidden mandible fracture? Isolated lateral pterygoid plate fractures noted on CT of the head may be suggestive of an unappreciated mandibular fracture. Liebert Pub Researchers found that in a case series, every patient with an isolated lateral pterygoid plate fracture also had an ipsilateral subcondylar or related mandibular fracture — meaning the two injuries are closely mechanically linked.
FAQ 13: How does the pterygoid process relate to the pterygopalatine fossa? The pterygopalatine fossa is a pyramidal space located posterior to the maxilla, anterior to the pterygoid process of the sphenoid, lateral to the perpendicular plate of the palatine, and inferior to the greater wing and body of the sphenoid. ScienceDirect This fossa is a critical neurovascular crossroads — it contains the maxillary nerve, the pterygopalatine ganglion, and the Vidian nerve, all of which have direct clinical significance.
FAQ 14: What role does the pterygoid process play in TMJ disorders? Poor coordination of the superior and inferior heads of the lateral pterygoid muscle can disrupt the position of the articular disc of the TMJ, which may contribute to temporomandibular disorders (TMD). Physiopedia Since the lateral pterygoid originates from the pterygoid process and inserts into the TMJ disc, dysfunction in this muscle directly implicates the bony structure in jaw pain, clicking, and restricted opening.
FAQ 15: How does pterygoid muscle spasm present clinically? The spasm of the lateral pterygoid muscle can be painful and result in trismus (locked jaw), and the patient may require analgesics or muscle relaxants. NCBI Medial pterygoid spasm similarly causes jaw stiffness and difficulty opening, and pain may radiate to the ear, throat, and TMJ — making it easy to misdiagnose as dental or ear pathology.
FAQ 16: What is a pterygoid implant in dentistry? Pterygoid implants are based on the implantation of an osseointegrated device within the pillar consisting of the maxillary tuberosity, the palatine bone, and the pterygoid process of the sphenoid bone, allowing anchorage into greater cortical bone surface and providing high stability. PubMed Central The technique was first described by Tulasne in 1989 and has become an important graftless option for the severely atrophied posterior upper jaw.
FAQ 17: What is the success rate of pterygoid implants? The pterygoid technique has been highly successful, with a 10-year cumulative survival rate of 92.5%. PubMed Central An earlier systematic review also reported a 92% short-term survival rate, comparing favorably with other approaches in the posterior maxilla and making it a reliable long-term rehabilitation option for suitable patients.
FAQ 18: What are the risks of placing a pterygoid implant? The pterygoid region is close to significant vascular structures such as the maxillary artery, and accidental injury to these vessels can cause severe bleeding. The posterior superior alveolar nerve and branches of the maxillary nerve run near the implantation site, and injury can result in paresthesia or anesthesia. Periobasics Maxillary sinus perforation and infection are additional recognized risks requiring careful surgical planning.
FAQ 19: How does the pterygoid process support the auditory tube? The pterygoid process with its lateral and medial plates and the pterygoid fossa on the undersurface of the skull provide surfaces of attachment for the masticatory muscles and give support to the auditory tube. Springer The medial plate in particular is closely related to the cartilaginous portion of the Eustachian tube, which is why pterygoid region pathology can sometimes cause ear symptoms.
FAQ 20: What is the scaphoid fossa of the pterygoid process? Above the pterygoid fossa is a small, oval, shallow depression called the scaphoid fossa, which gives origin to the tensor veli palatini. Wikipedia This muscle, which tenses the soft palate, begins here before its tendon descends to wrap around the pterygoid hamulus — a critical arrangement for normal swallowing and middle ear function.
FAQ 21: What does the pterygoid process look like on a CT scan? On axial CT slices, both plates of the pterygoid process appear as distinct bony shelves flanking the pterygoid fossa at the base of the sphenoid. Thin-slice high-resolution CT imaging is the gold standard for diagnosing facial fractures and making decisions for treatment Digital Diagnostics in this region. The pterygoid canal is best seen on axial cuts just above the plate level as a fine anteroposterior bony tunnel running through the root of the process.
FAQ 22: How is the pterygoid process involved in Le Fort I orthognathic surgery? The most critical factor for successfully performing setback and superior/posterior impaction of the maxilla in orthognathic surgery is securing sufficient space, which can be achieved through pterygoid plate fracture, removal, or grinding. PubMed Central The pterygomaxillary junction — where the maxilla meets the pterygoid plates — must be properly separated during Le Fort I osteotomy to allow the jaw to be repositioned safely and stably.
FAQ 23: What is the pterygomasseteric sling and how does it relate to the pterygoid process? The medial pterygoid muscle along with masseter muscle forms a “pterygomassetric sling” that suspends the mandible. NCBI Because the medial pterygoid originates from the pterygoid process of the sphenoid, this sling is directly anchored to it. Disruption of the pterygoid plates — whether from trauma or surgery — therefore affects the entire force-generating sling and mandibular stability.
FAQ 24: Why is the pterygoid process important in surgical approaches to the skull base? The pterygoid process marks the anterior boundary of several critical skull-base spaces. Tumors can develop silently in the retromaxillary space because of their concealed location, and the medial surface of the medial pterygoid plate grossly demarcates the retromaxillary space from the nasopharynx. Springer Surgeons performing endoscopic skull-base procedures, infratemporal fossa dissections, or Vidian neurectomies must have precise knowledge of this structure to avoid catastrophic vascular or neural injury.